| Muscle | Origin | Insertion | Innervation | Action |
|---|---|---|---|---|
| Anterior scalene | Anterior tubercle of TP of C3-C6 | Scalene tubercle of 1st Rib | Anterior Rami C4 - C6 |
Mobile ribs: Elevates ribs during forced inspiration Fixed ribs (unilateral): I/L C/s sidebend (unilateral) Fixed ribs (bil): C/s flexion, Cervical lateral stabilization |
| Middle scalene | C1-C2 TP Posterior tubercle of TP of C3-C7 |
1st Rib (posterior to groove for subclavian a.) | Anterior Rami C3 - C8 |
Mobile ribs: Elevates ribs during forced inspiration Fixed ribs (unilateral): I/L C/s sidebend (unilateral) Fixed ribs (bil): C/s flexion, Cervical lateral stabilization |
| Posterior scalene | Posterior tubercle of TP of C5-C7 | 2nd Rib (outer surface) | Anterior Rami C6 - C8 |
Mobile ribs: Elevates ribs during forced inspiration Fixed ribs (unilateral): I/L C/s sidebend (unilateral) Fixed ribs (bil): C/s flexion, Cervical lateral stabilization |
Scalene Muscles
Origin
The scalenes originate distally. The anterior and middle scalenes originate from the 1st rib2,4. The posterior scalene originates on the outer surface of the second rib4.
Insertion
The scalene muscles can be broadly considered to insert proximally on the transverse processes (TP) of C2–C72.
As one can see in Table 1, each scalene individually varies on which vertebrae it inserts on and what parts of the TP.
Action
When contracting, the scalenes are considered to have the same action.
Fixed ribs
When the ribcage is fixed, unilateral contraction of the scalenes results in ipsilateral sidebend cervical spine2,4.
Bilateral contraction in this environment results in cervical spine stabilization against lateral movement2 and cervical flexion4.
Mobile ribs
When the ribcage is free to move, bilateral contraction of the scalenes results in elevation of the first and second ribs to assist in forced inspiration2,4
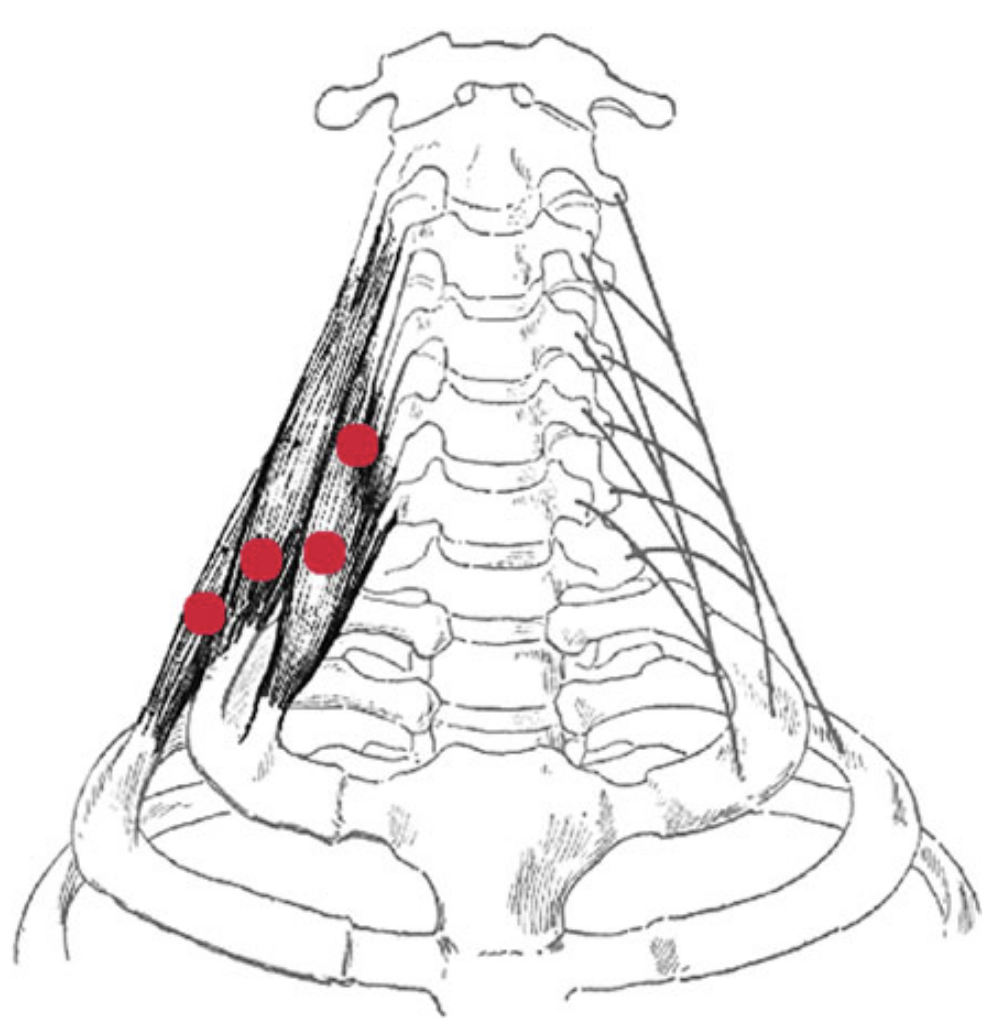
Palpation
To palpate the scalenes, you must identify:
- Thyroid cartilage
- Located along the anterior midline of the neck.
- The superior border of the thyroid cartilage, the Adam’s apple, lies anterior to C4; the distal border of the thyroid cartilage lies anterior to C5.
- The thyroid cartilage can be observed moving up and down during swallowing.
- Hyoid bone
- Located above the thyroid cartilage and lying horizontally.
- The hyoid bone is the first bony structure to be palpated as you move downward along the midline from the mandible.
- It can be palpated as it moves up and down during swallowing.
- The hyoid bone lies anterior to C3.
- External jugular vein
- Begins near the angle of the mandible, crossing the sterno cleidomastoid in the superficial fascia before passing posterior to the posterior border of the muscle, to empty into the subclavian vein.
- In the healthy patient, lying supine, the vein is clearly visible only a short distance above the clavicle.
- However, with increased thoracic pressure (noted in pathologies such as heart failure, enlarged supraclavicular lymph nodes, and obstruction of the superior vena cava) the external jugular vein becomes prominent throughout its course.
- Sternocleidomastoid muscle
“The scalenes can be palpated when they are constricted or harbor trigger points. Note the location of the external jugular vein where it crosses the sternocleidomastoid: constriction of the anterior scalene can be palpated just deep to this area. Move the palpating finger slightly posteriorly to this area to locate the scalenes; they will feel like taut bands if they are constricted. It is essential to palpate this area with the greatest sensitivity to patient tenderness and discomfort. An extremely gentle touch is required to be able to palpate the muscle without causing pain to the patient.”2
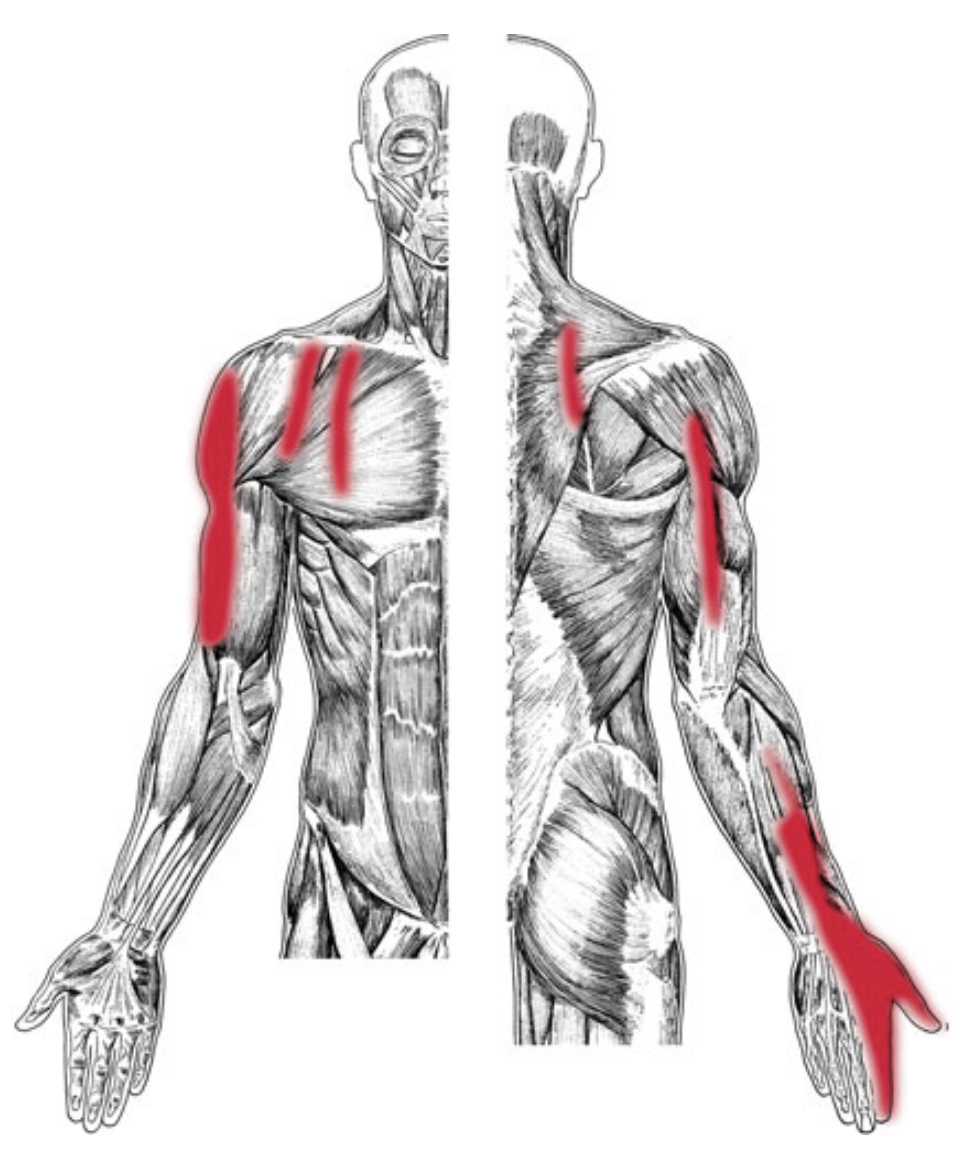
Pain pattern
“Pain pattern: Persistent, aching pain that radiates anteriorly and downward toward the chest in fingerlike projections and/or laterally to the upper arm. Pain may skip the elbow and reappear at the radial side of the forearm, hand, thumb, and index finger. Pain may radiate posteriorly into the midscapular area.”2
Etiology
Satellite trigger points
Affected Organ System
When the scalenes are dysfunctional and have trigger points, generally the respiratory system is affected as well2.
Associated zones, meridians, and points
Release
Stretching
NPTE Stretching Recommendation
“Look over your scalenes”
- Ipsilateral rotation
- Contralateral sidebend
- Neck extension
“Laterally bend the head and neck so that the ear of the unaffected side moves toward the same shoulder. Hold for a count of ten. Then, without changing the degree of lateral stretch, rotate the head and face toward the affected side, stretching the cheek toward the ceiling. Hold for a count of ten. Return the head and face to the initial lateral stretch position. Now rotate the head and face, this time aiming the chin in toward the clavicle. Hold for a count of ten. Return the head and face to the initial lateral stretch position.”2



References
1.
Donnelly JM, Simons DG, eds. Travell, Simons & Simons’ Myofascial Pain and Dysfunction: The Trigger Point Manual. Third edition. Wolters Kluwer Health; 2019.
2.
Finando D, Finando SJ, Finando D. Trigger Point Therapy for Myofascial Pain: The Practice of Informed Touch. Healing Arts Press; 2005.
3.
Neumann DA, Kelly ER, Kiefer CL, Martens K, Grosz CM. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation. 3rd ed. Elsevier; 2017.
4.
Gilroy AM, MacPherson BR, Wikenheiser JC, Voll MM, Wesker K, Schünke M, eds. Atlas of Anatomy. 4th ed. Thieme; 2020.
Citation
For attribution, please cite this work as:
Yomogida N, Kerstein C. Scalene Muscles. https://yomokerst.com/The
Archive/Anatomy/Skeletal Muscles/Head and Neck/Neck Muscles/Scalene
muscles/scalene_muscle_group.html